
Overview // The Challenge // Methodology // The Team // Tools // Process // Final Deliverables // Key Learnings // Testimonials //

Watch a short film documenting the final research stages and design concept below.
Project: Hearticulate (previously known as WomenToHeart)
Competition: Winner of the pan-European Student Service Design Challenge 2020
Project Sponsors: Service Design Days, Philips Experience Design, IBM, Ellen McArthur Foundation
Team members: Angela Tam, Maria Domeyko, Laura Duarte, Ruchika Karnani, Katerina Shikhotova
Project Duration: 5 month research to design output; resulting in a 3 month internship at Philips Experience design to further develop the winning concept.
My role: Design Researcher, Design Strategist, Illustrator, Videographer, Service Designer, Narrative Storyteller
Skills Strengthened: Adaptive Research Methods, Research-Led Human-centred Design, Developing User Flows and Wire-Framing, Remote Team Collaboration, Designing for Complex Systemic Problems
Project output: Digital Preventative Health Service for women
The Challenge
This project was conceived as a submission to the Student Service Design Challenge 2020. The brief aimed for student groups to uncover problems and solutions that could improve the heart health of different demographics in Europe who are “‘invisible’, neglected, underserved, forgotten or overlooked.”
While defining our focus, our team discovered that heart disease is the number one killer in women worldwide. Yet only one in three women are aware of it. After recognising that half of the world’s population is underserved due to a system of challenges including public awareness, gaps in medical research and diagnostics, and medical biases, we were called to dig into this complex problem.
Our research question became…
How might we help women to recognize the symptoms of a heart attack and to seek help in a timely manner?
Methodology
The competition was structured against 4 steps of the design process and was driven by several design frameworks such as Cocreate by Philips Experience Design, the Double Diamond, Design Thinking and Enterprise Design Thinking by IBM. Each stage was assessed by the jury consisting of members of Philips, IBM, Service Design Days and Ellen McArthur Foundation.

Project timeline and methodology
The Team
Our team comprised of 5 women, from 5 different countries around the world, and varying professional and academic backgrounds, from graphic design and architecture, to international relations and employee engagement, who had all converged in the field of service design. This allowed us to extrapolate from a diverse breadth of experience and perspective, and not only to play to our strengths but also learn from one another. At different times, we leaned on one another to take the lead on specific tasks and project management.

Tools

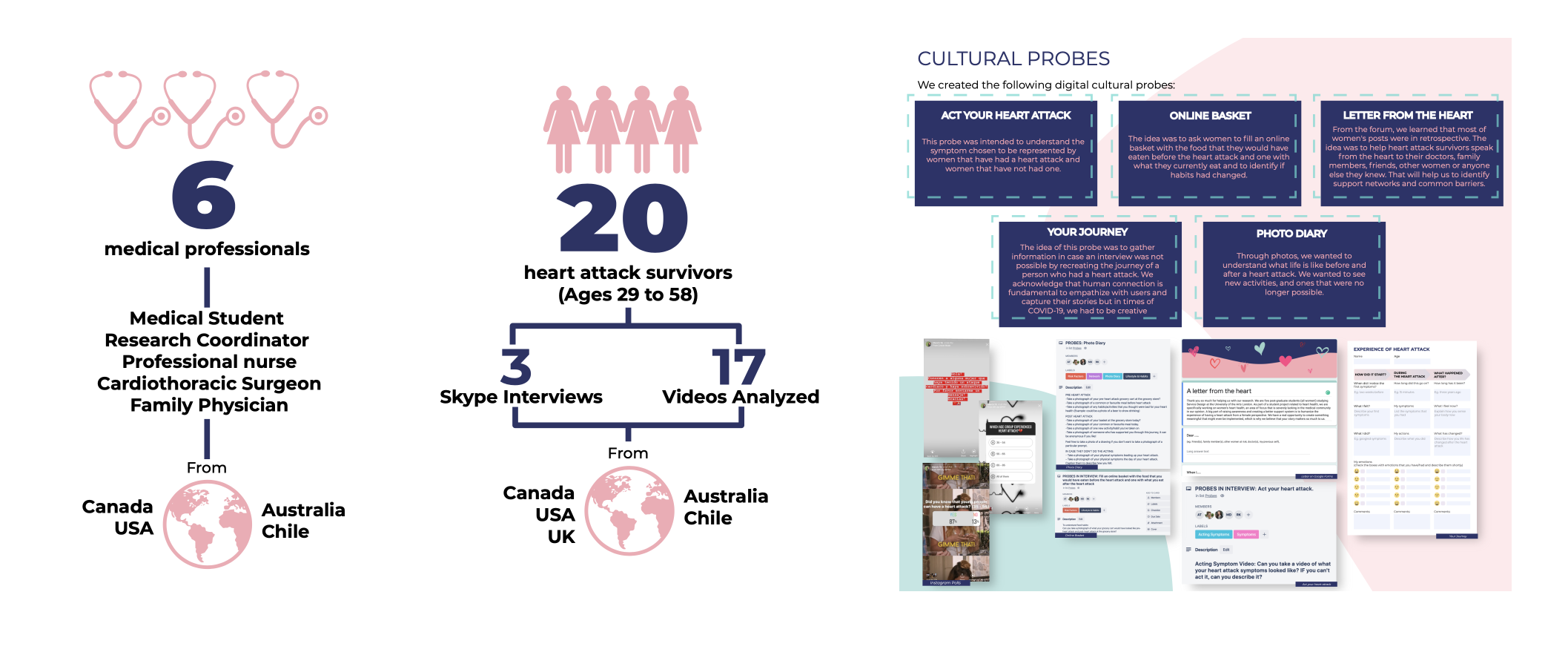
We had to pivot project plans, research methods, ways of working and communication to work together under these new uncertain circumstances. We recognised that our primary research audience, women heart attack survivors, were particularly vulnerable to COVID and it would no longer be safe to reach them in physical contexts. Therefore, we adapted conventional tools and found creative means to conduct research and interact with our audience. We invented and iterated on new ways to reach out to all stakeholders, conscious that many medical experts at this moment would be overstretched and unable to have long conversations with us. We created digital cultural probes, surveys, and instagram polls as means to engage with our desired users and experts.
Despite challenges, we managed to better our project by reaching out to our global networks beyond the initial UK scope, and were able to maintain a human-centred, iterative and collaborative approach. We adapted quickly to working online, using tools like Miro, Whatsapp, Slack, and Trello to communicate, coordinate, and continue to design together. We learned to be accountable and over-communicate when working independently while half the team was sleeping across the world, making the most of limited face-to-face group meetings.
Process
Stage 1: Identify and Explore
In our first exploration, we were shocked to find out that heart disease is the number one killer in women, but we were even more surprised that it wasn’t common knowledge. Through desk research, we discovered that heart attacks don’t fit the stereotype of a middle aged man clutching his chest, but they can happen to anyone and be expressed in a wide range of symptoms that are often left un-assessed by doctors.
Here are the problem areas we discovered.

However, it is not commonly known that so many women are affected by this problem. Historically, heart disease has been perceived as a "male disease". Because of this discrepancy, many women are unaware of their risks and how heart attack symptoms may be presented in their own bodies.

“Only one third of cardiovascular clinical trial subjects are female and only 31% of cardiovascular clinical trials that include women report results by sex”- 2014 Brigham and Women’s Hospital report

Men and women can suffer from different heart attack symptoms and these symptoms can present months prior to the actual cardiac event in women.

According to the research of the British Heart Foundation, women are 50 per cent more likely to receive a wrong initial diagnosis when they are having a heart attack. That increases their risks of dying by 70 per cent.
To corroborate these findings and to test our assumptions, we utilised cultural probes, asked women to act out heart attacks for us, and conducted surveys on social media.
Stage 2: Empathize and Explore
COVID was a shock to the world and traditional methods of conducting primary research with users became infeasible due to lockdown. Instead of giving up, we reached outwards online - to facebook groups, heart health forums, medical professionals and even personal contacts, our collective networks spanning hundreds of people. We realised that in order to understand the barriers faced by women who might struggle to seek help for a heart attack, we should first speak to women who have had heart attacks to better understand their experiences. Because this was a particularly hard to access audience, we relied on creative methods to collate research.
To uncover more stories of heart attack survivors, we combed the internet for online blogs, videos, news articles and documentaries to connect similar challenges and gaps in the system.
We conducted in-depth and expert interviews, and created several online cultural probes for women and heart attack survivors to interact with.
Through our interviews, we gained the following insights:
Heart attacks can often present as less severe conditions in women, such as heartburn and panic attacks, and can be misdiagnosed by women themselves AND doctors.
Women can exhibit low level symptoms for months leading up to a heart attack.
It is common for women to experience angina while resting, and not just while exerting themselves physically.
Women who experience classic symptoms seek help sooner than those who experience vague and slow-onset symptoms, increasing their risks of heart damage. “Heart attack symptoms in women are often built slowly and unfortunately, heart attacks depend 100% on how long a person waits to get treatment. The faster you react, the less your heart dies”. Isidora López (Chilean nurse)
Stage 3: Frame and Define
After stepping back and analyzing all of our research as a whole, we recognised a system that was broken each step of the way…

Once we were able to narrow our areas of focus, we clearly saw 3 areas of opportunity that we could act within.

Stage 4: Ideate and Develop
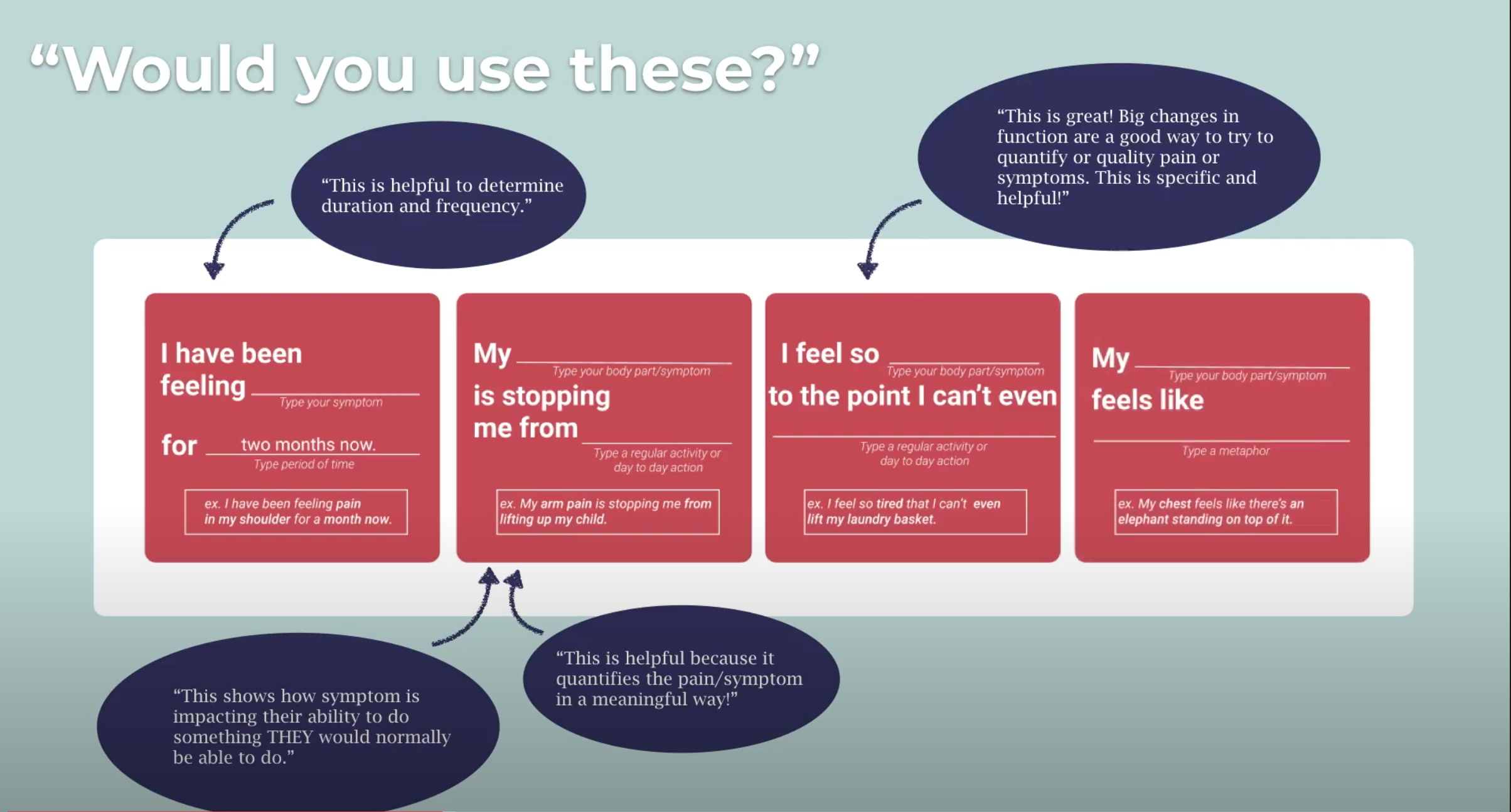
We found that women often had trouble describing their symptoms in a concise way that would alarm their doctor of an impending heart attack. Doctors agreed it was often hard for patients to describe their conditions and existing pain scales are not accurate. After analysing many stories of women heart attack survivors sharing their experiences in their own words, we noticed that the most impactful symptom descriptions were the ones that used metaphors.
Challenged to address this communication gap between women and medical staff, we developed a set of prompts that could help women to use descriptive yet concise language to describe their symptoms, testing each prompt with the medical community to ensure usefulness in diagnosis. The results were overwhelmingly positive.
After several individual and group ideation sessions, we developed a series of prototypes to test with users.

Finally, we got our aha moment when talking to Carolyn Thomas, a mayo-clinic trained women’s heart advocate who also happens to be a heart attack survivor, who has supported our research throughout…
“There are people doing awareness, there are people doing forums, there is no one showing women how to communicate their symptoms with their own words”.
We tested the prompts with medical professionals and heart attack survivors. 95% of women experience early warning signs, also called prodromal symptoms, in the weeks or months prior to a heart attack. In fact, women who experienced one or more of five most common prodromal symptoms are FOUR TIMES more likely to have an adverse cardiac event. Therefore, our main service not only works for women at high risk of having a heart attack but for those who are experiencing these symptoms while continuing on with their lives.
We used Miro to map out the user flow, blocking out what content needed to be shared and where it should go. After countless iterations and feedback with potential users and one another, we then moved to develop the final prototype in Figma.
Insights to Action



Final Deliverables

Impact
The project was unanimously chosen by the jury to win the Student Service Design Challenge 2020.
The team presented the project at Dutch Design Week 2020 at the opening speech, a design panel with Philips Chief Design Officer Sean Carney, and exists within an online exhibition within the DDW website.
The team continued revising and expanding on the project during the Design-in-Residence programme at Philips Experience Design, building our understanding in different realms of design, such as design strategy, UX and Usability, brand and communication, and more.
Key Learnings
How to distill a huge problem into something tangible
When we first began working on this brief, we struggled to narrow down the scope. While others recommended that we choose women with particular risk factors to make our primary user more specific, we knew we wanted our design to challenge this idea that only women with risk factors can have heart attacks. Once we discovered the system of challenges facing women, we created many prototypes addressing multiple opportunity areas. The most important one for us was awareness, but public awareness and finding a large enough audience to reach critical mass is difficult. Instead, we went back to our research and chose to focus our design concept on the most important insights that we could make a difference within, namely communication between women, their support systems, and medical professionals, and it was impactful because our final outcome had been entirely research-led and it had clear potential for tangible positive impact.
Working collaboratively with a fully remote team
While working remotely was not always easy and we terribly missed collaborating together in one room, I learned valuable methods and experiences on how to successfully navigate working on a fully remote team, where no one was in the same time zone. This is a valuable skill to have as it has proven to myself that I will have no problem adapting to the future of work where our physical locations may no longer be barriers to joining exciting projects around the world. Often we would manage individual tasks, break into pairs for collaboration, and. An important lesson I learned from this experience is to trust your team to complete their tasks without trying to do everything on your own or together. If we had wanted to do each task “together”, we would have never gotten anything done trying to co-ordinate the right times to meet. Instead, we trusted one another to do good work, and then elevated one another by taking the time to review and give feedback. Based in the “latest” time zone on the west coast, I would often wake up to hundreds of notifications and comments, and would spend the first hour or two of my day catching up and feedbacking on my team’s work. While it may seem tedious, it ensured the highest quality of our work to remain highly collaborative and nuanced.
Pivoting and Adapting to Challenges
This project was filled with challenges, from having each of our lives in London uprooted or disrupted by the pandemic, to working completely remotely on different time zones. Not just that, we had to entirely rethink our project scope, research methods, modes of engagement, and how we could reach our research audience virtually. For myself, as a perpetual night owl, shifting to early mornings, with meetings often slated for 5am etc, it was exhausting. However, I learned that I am able to rise to the challenge, and am even capable of articulating myself clearly at panel discussions at 4 in the morning! Within each obstacle, we didn’t shrink down but instead persevered and grew resilience.
Testimonials
“I would definitely send this out to my readers as a resource they could use if this became a real project.” - Carolyn Thomas, Founder of Heart Sisters heart health blog and heart attack survivor
“I totally support the work you are all doing and would be happy to help you with anything further and to promote this service at my heart clinic when it is ready.” - Janneke Wittekoek (leading women’s heart health cardiologist; founder of Heartlife)
“Well researched with input from many subject matter experts leading to a great ‘aha’ moment and problem to solve. The story of the problem and solution are well told and the tools and guidance provided in the product are a pleasure to use.” - Rosie Martin, Design Principal at IBM
“Ticks all the boxes from a highly relevant underserved population to a great concept and great storytelling.” - Sean Carney, Chief Design Officer of Philips
“The team shaped a strong solution in the context of preventive care where digital technology enables effective inclusion and peer-to-peer support in contemporary society.” - Simona Maschi, co-founder and director of the Copenhagen Institute of Interaction Design (CIID)